The Executive Artery Crisis: Why Fasting LDL-C Misses the Mark on Business Dinners
Frequent corporate dining creates an invisible cardiovascular crisis. Discover why postprandial hyperlipidemia and sdLDL render standard fasting cholesterol tests insufficient for high-performers.

Executive lifestyles characterized by frequent business trips and corporate dinners mask a silent arterial crisis, driving premature cardiovascular events despite seemingly normal health checks. According to clinical guidelines and insights supported by the World Health Organization and the Malaysia Ministry of Health, relying solely on basic lipid panels leaves high-performing professionals exposed to acute cardiovascular incidents nearly a decade earlier than regional averages.
| Key Dimension | Clinical Standards & Data Context | Business Impact |
|---|---|---|
| Onset Age Gap | ACS average age in Malaysia is 58.7 (10 years earlier than Singapore); 25% are < 50. | Catastrophic loss of executive leadership during peak productivity years. |
| Residual Risk | 36.7% ACS prevalence in MY with average LDL-C of 3.1 mmol/l at admission. | ”Normal” LDL levels provide false security; hidden productivity and mission-critical risk. |
| Intervention Target | < 26% carb energy; 5-10% weight loss; Asian BMI < 27.5 kg/m². | Direct ROI in sustaining cognitive stamina and long-term leadership continuity. |
1. Patient Misconceptions: The “Elite Diet” and Fasting LDL-C Myths
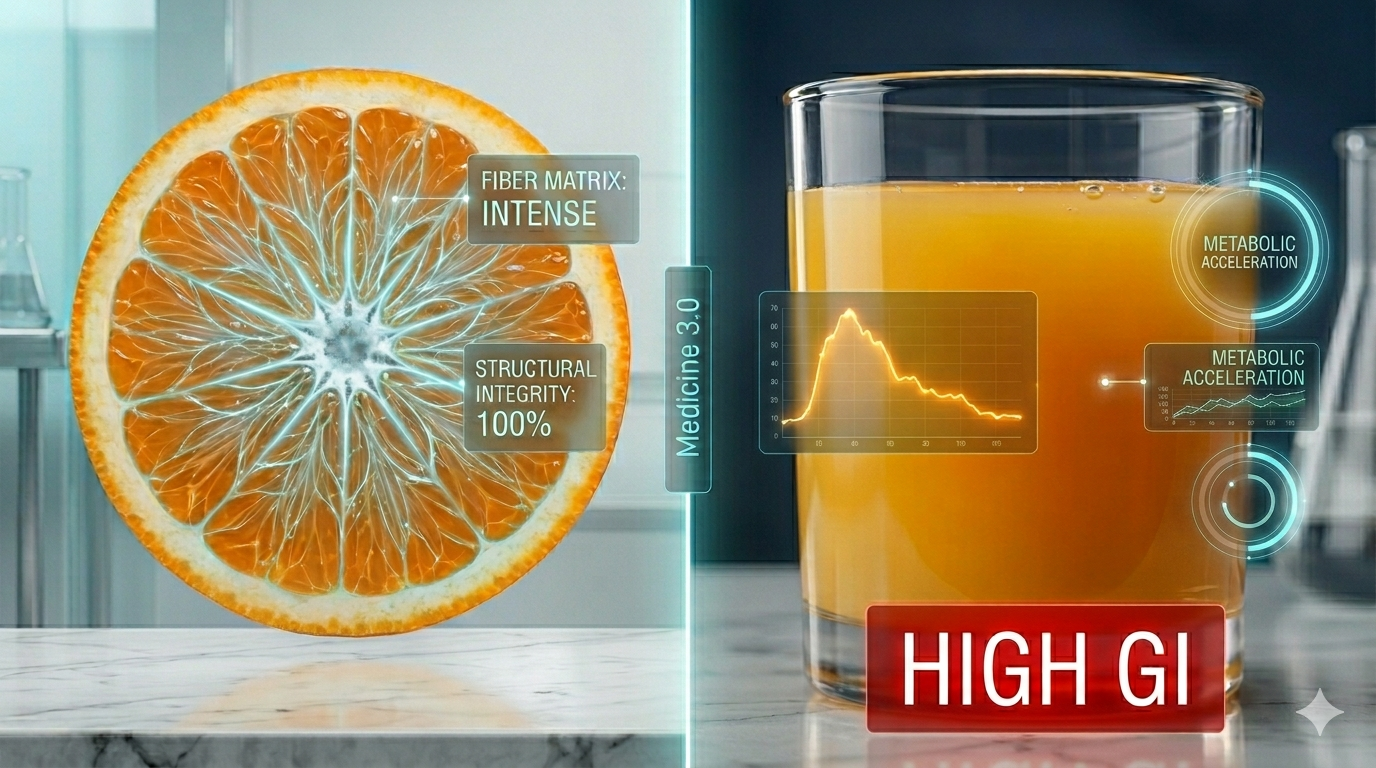
Normal fasting LDL-C does not guarantee arterial health; frequent corporate dining causes postprandial hyperlipidemia, exposing vessels to highly atherogenic small dense LDL (sdLDL) and remnant particles.
Many executives believe adopting a “low-carb, high-protein” diet during business dinners fully mitigates metabolic risks. They assume that if their annual health screening shows a normal fasting LDL-C, their cardiovascular system is secure. However, a defining feature of Atherogenic Dyslipidemia in corporate professionals is Postprandial Hyperlipidemia—transient but severe spikes in blood lipids following heavy meals.
Because of continuous metabolic loading, the vascular endothelium is chronically exposed to a dominant distribution of small, dense Low-Density Lipoprotein (sdLDL) particles. These sdLDL particles easily penetrate the arterial wall and oxidize, accelerating plaque formation. Medicine 3.0 principles emphasize that Non-HDL-C (Total Cholesterol minus HDL-C) encompasses all atherogenic particles, making it a far superior risk predictor compared to fasting LDL-C alone as documented in PubMed.
2. Medical R&D Frontiers: Addressing Residual Risk and ApoB
Even when standard LDL-C reaches therapeutic targets, substantial residual risk remains due to elevated Lipoprotein Remnants and ApoB particles, driving early-onset heart disease.
Modern medical R&D has shifted toward solving “residual risk.” Clinical data shows that in Malaysia, the average age for an Acute Coronary Syndrome (ACS) event is 58.7 years—10 years earlier than in Singapore. Shockingly, 40% of these ACS patients already carry more than 3 traditional cardiovascular risk factors.
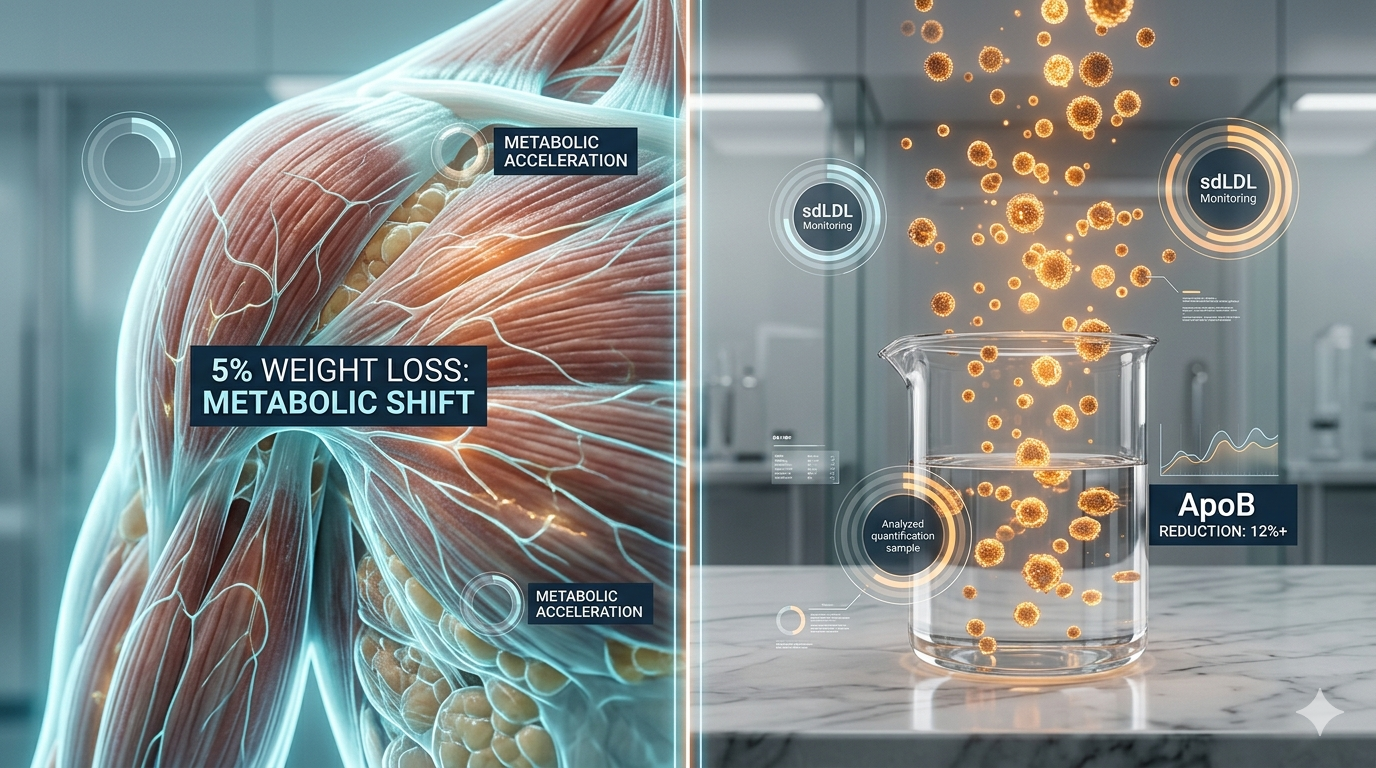
This paradox is explained by Remnants (triglyceride-rich lipoprotein remnants) and sdLDL. Even when statin therapy lowers total LDL-C volume, the sheer number of atherogenic particles remains dangerously high. This is why tracking ApoB (Apolipoprotein B) has become a non-negotiable metric. Every atherogenic particle contains exactly one ApoB molecule, providing a precise count of the actual threats in your bloodstream, rather than just estimating the cholesterol payload.
3. Daily Prevention Focus: Reversing Atherogenic Dyslipidemia
Reversing insulin resistance through targeted 5-10% weight loss and strictly limiting carbs to < 26% shifts dangerous sdLDL into benign, buoyant particles.
Proactive health strategies for executives must pivot from monitoring single nutrients to managing holistic dietary patterns and metabolic health. Atherogenic dyslipidemia is deeply intertwined with insulin sensitivity. By optimizing insulin resistance, professionals can fundamentally halt the overproduction of sdLDL at its source.
Clinical guidelines from the Singapore Ministry of Health and Malaysia MOH emphasize achieving a minimum of 5-10% weight loss for significant lipid profile improvement. Furthermore, a diet with < 26% total energy from carbohydrates has been proven to physical alter LDL particle size. Combined with managing waist circumference (target: < 90 cm for men, < 80 cm for women) and maintaining a healthy Asian BMI below 27.5, these daily focuses build impenetrable cardiovascular resilience.
💡 VitalsTrack Medicine 3.0 Zero-Friction Assessment: Every CTA must explicitly state: “No app download required. Reply with keywords or send photos directly via WhatsApp/Telegram.” Users can experience VitalsTrack’s core services (lab report analysis, diet evaluation, and exercise heart rate calculation) using their most familiar messaging tools, driving a quantum leap in conversion rates.
Q1: Why did I have a cardiovascular event if my fasting LDL-C was in the normal range?
Answer: Normal fasting LDL-C only measures total cholesterol content, not the number of particles. Conditions like postprandial hyperlipidemia and high levels of sdLDL or Remnants—often triggered by frequent heavy meals—create a highly atherogenic environment that standard tests miss.
Q2: What is the most accurate test for cardiovascular risk?
Answer: Medicine 3.0 protocols recommend testing for ApoB and Non-HDL-C, as they measure the actual count of all atherogenic particles (VLDL, IDL, LDL) rather than just the weight of the cholesterol they carry.
Dual-City Strategic Medical Liaison
- Kuala Lumpur: The Exchange TRX, Level 33
- Singapore: Novena Medical Center, Suite 11-04