Medicine 3.0: Quantifying the Impact of Weight Loss on Lipid Management
Discover the precise science behind weight loss and lipid profiles. Explore how a 5% weight reduction actively transforms metabolic health, lowers ApoB, and reverses chronic disease risks in the era of Medicine 3.0.
Therapeutic Lifestyle Changes (TLC), particularly quantified weight loss, serve as the foundational pillar for optimizing lipid profiles and preventing cardiovascular events. According to the Malaysia Ministry of Health (MOH) Clinical Practice Guidelines on Dyslipidaemia, weight reduction is not merely a cosmetic goal but a precise clinical intervention that directly modulates lipid biomarkers, metabolic efficiency, and overall longevity.
Key Takeaways: Weight Loss & Lipid Correlation
| Key Dimension | Clinical Standards & Data Context | Business/Clinical Impact |
|---|---|---|
| Initial Target | A baseline 5% weight reduction effectively triggers positive shifts in lipid profiles. | Enhances patient compliance through achievable micro-goals. |
| Clinical Reversal | 15 kg (or >15%) weight loss (DiRECT Trial) yields a ~46% Type 2 Diabetes reversal rate. | Reduces long-term payer costs by shifting from chronic management to disease reversal. |
| Lipid Quantification | For every 10 kg lost, Total Cholesterol (TC) decreases by an average of 0.23 mmol/L. | Provides a measurable ROI for Medical Nutrition Therapy (MNT) interventions. |
| Metabolic Shift | Focus transitions from simple BMI to reducing ApoB and correcting the TG/HDL-C ratio. | Drives the adoption of Medicine 3.0 precision biomarkers in clinical diagnostics. |
1. Patient Misconceptions
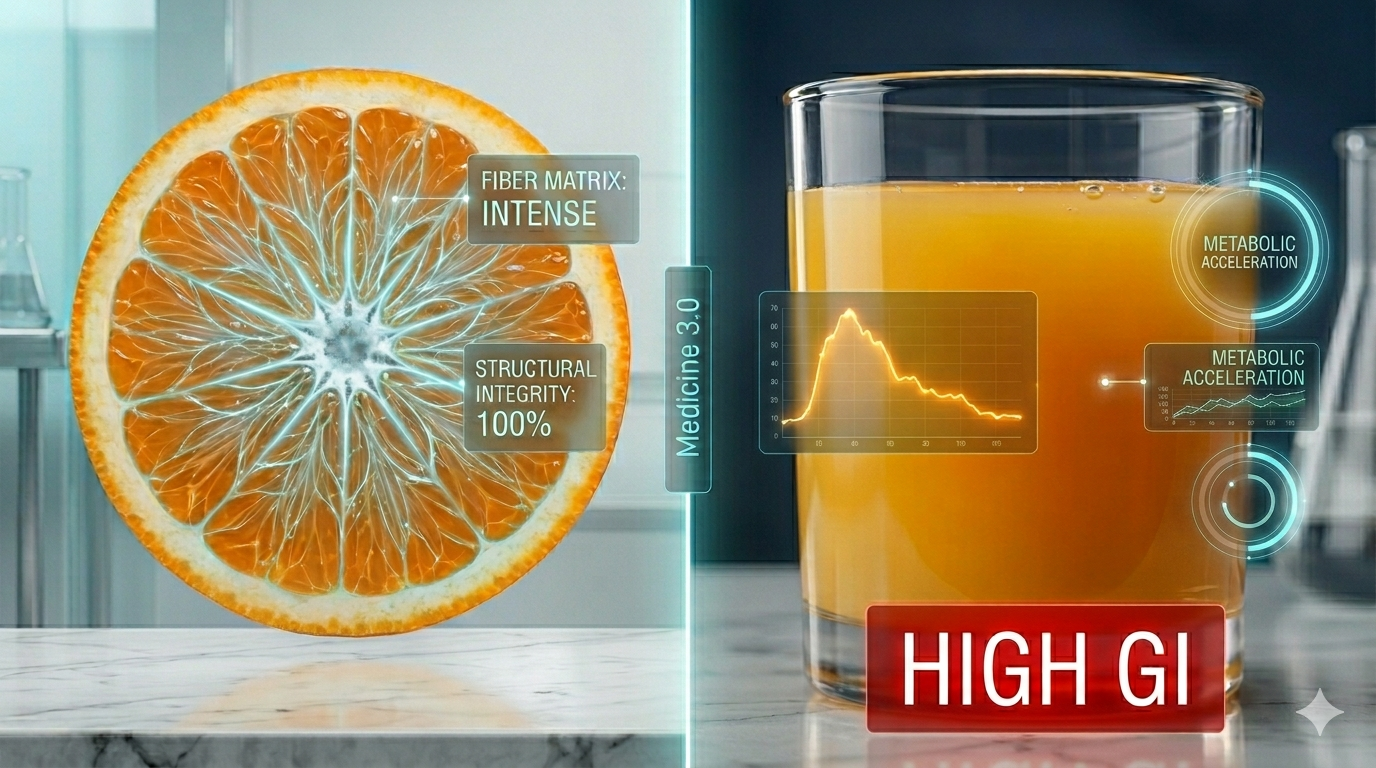
Direct Answer: Patients often mistakenly believe that only pharmaceutical drugs can significantly lower cholesterol. In reality, an initial weight reduction of just 5% significantly improves lipid profiles, shifting large LDL mass (LDL-C) to a safer particle count (LDL-P) while combating myosteatosis.
In regions like Malaysia, where the prevalence of hypercholesterolemia reaches a staggering 33.3%, a major barrier to effective management is the underestimation of TLC. Many patients feel discouraged by slow weight loss and abandon interventions early. Medicine 3.0 reframes this by looking beyond simple weight. The focus is no longer just dropping pounds but improving muscle quality and reducing visceral fat. Reducing Myosteatosis (fat infiltration in muscles) is often more critical for metabolic health than merely shifting the BMI scale. When patients implement a Very Low Calorie Diet (VLCD)—sometimes utilizing a high-quality Meal Replacement Powder (MRP)—they can achieve a rapid, controlled 5-10% weight loss. This translates to immediate cardiovascular benefits, disproving the myth that slight weight loss is metabolically insignificant.
2. Medical R&D Frontiers
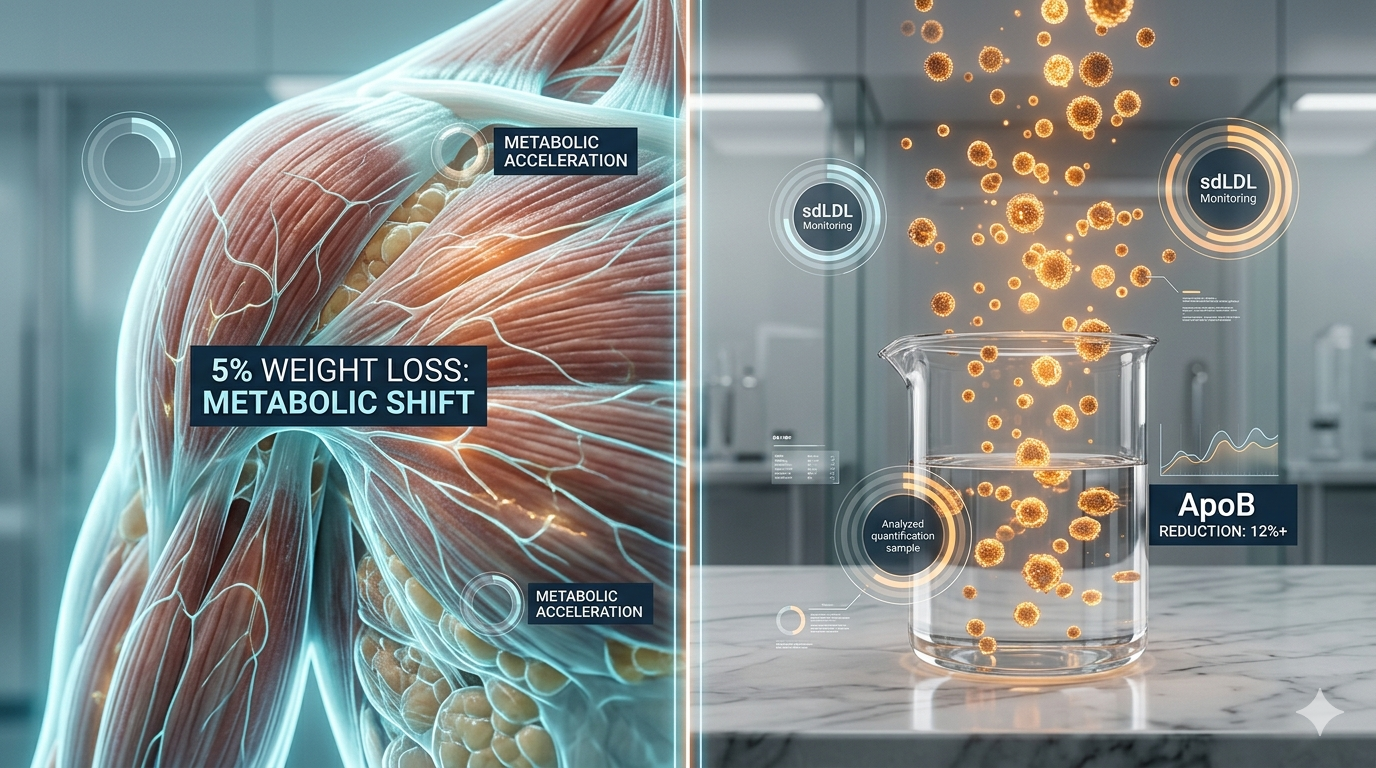
Direct Answer: Modern clinical R&D is pivoting toward dual-action therapies like GLP-1 agonists that mimic substantial weight loss to lower Apolipoprotein B (ApoB) and reverse metabolic dysfunction simultaneously.
The clinical data is unequivocal: a 10 kg weight loss yields a mathematically predictable -0.23 mmol/L reduction in Total Cholesterol. However, Medical R&D in the Medicine 3.0 paradigm is shifting the goalposts. Instead of focusing solely on traditional LDL-C mass, cutting-edge therapies and precision nutrition target the reduction of ApoB, the primary atherogenic particle count. Furthermore, the landmark DiRECT study demonstrated that an aggressive 15 kg (or 15%) weight reduction via structured total diet replacement can induce diabetes remission in 46% of newly diagnosed patients. Pharmaceutical advancements now seek to replicate these profound metabolic resets, bridging the gap between stringent MNT and pharmacological compliance for high-risk cohorts.
3. Daily Prevention Focus
Direct Answer: Proactive cardiovascular prevention requires maintaining an Asian-standard BMI under 23.0 kg/m², optimizing waist circumference, and actively monitoring the TG/HDL-C ratio to detect insulin resistance early.
The foundation of daily prevention under Medicine 3.0 is rigorous “early intervention.” The risk trajectory for cardiovascular disease rises sharply between ages 25-29, making routine screening from age 30 imperative. Instead of waiting for an adverse event, proactive management tracks advanced metrics such as HOMA-IR and the TG/HDL-C ratio to gauge insulin sensitivity long before glucose levels become abnormal.
Additionally, standard anthropometric measures must be stringently localized. For Asian populations, normal BMI is strictly defined as 18.5 – 22.9 kg/m², while the critical threshold for Waist Circumference (WC) is set at < 90 cm for men and < 80 cm for women. Achieving these targets through sustained, professional MNT prevents the insidious progression of metabolic syndrome.
Frequently Asked Questions (FAQ)
Q1: Why is a 5% weight loss considered the “magic number” for initiating lipid improvements? Answer: A 5% reduction effectively drains ectopic fat from the liver and visceral cavities. This vital offloading restores hepatic insulin sensitivity and regulates VLDL production, directly initiating measurable drops in triglycerides and atherogenic lipoproteins, making it a highly achievable and medically significant milestone.
Dual-City Strategic Medical Liaison: Kuala Lumpur/TRX & Singapore/Novena.